Just five years ago, the word "Ozempic" was unknown outside of endocrinology clinics. Today, it appears in newspaper headlines, WhatsApp conversations, and TikTok's trending topics. Semaglutide —the active ingredient behind Ozempic and Wegovy— has sparked an unprecedented debate about what it means to lose weight, what it means to be hungry, and what role nutrition should play when a drug can silence appetite in ways willpower never could. But alongside the enthusiasm, a growing concern is emerging among nutritionists and physiologists: not all the weight loss produced by these medications is fat. A significant portion, as clinical trials show, can be muscle.
What Are GLP-1s and Why Have They Changed the Game
GLP-1 (glucagon-like peptide-1) is a hormone naturally produced by the body after eating. Its job is multifaceted: it stimulates insulin release, inhibits glucagon, slows gastric emptying, and, crucially, sends signals to the brain to indicate satiety. GLP-1 receptor agonist drugs —semaglutide (Ozempic, Wegovy), liraglutide (Saxenda), and tirzepatide (Mounjaro)— mimic and amplify this signal in a sustained manner, far beyond what the natural hormone can do on its own.

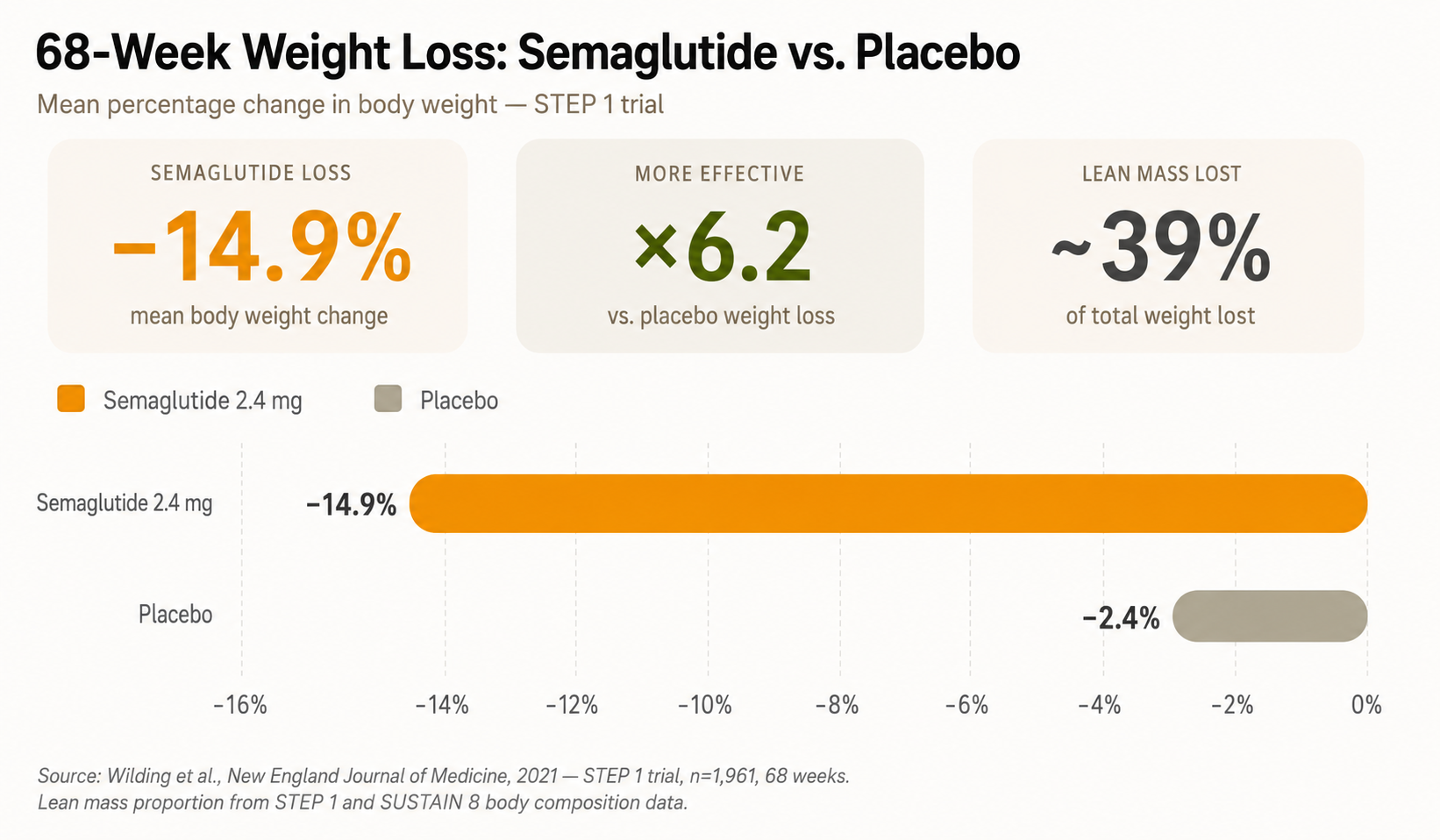
What makes these drugs special is not just their efficacy —the STEP 1 trial showed that semaglutide 2.4 mg reduced body weight by an average of 14.9% compared to 2.4% for placebo over 68 weeks, with lifestyle supervision in both groups— but the type of experience they create for those who take them. Patients don't talk about "eating less with effort." They talk about something deeper: hunger, as they knew it, simply disappears. And for many people who have been struggling with weight for decades, that can feel transformative.
Hunger Rewritten: What Really Changes in the Brain
The human experience of hunger is extraordinarily complex. It's not just an empty stomach: the hypothalamus, the dopaminergic reward system, the vagus nerve, and dozens of hormones are involved in a constant dialogue. GLP-1s act especially in the area postrema and the arcuate nucleus of the hypothalamus, regions that regulate homeostatic appetite, but they also affect the nucleus accumbens —the brain's pleasure center—, reducing the emotional appeal of highly palatable food.
The result is that many users describe how foods that were once irresistible —a pizza, an ice cream, a bag of potato chips— simply lose their power over them. It's not that they are making an effort to resist: it's that the desire has diminished. For many people with chronic obesity who have struggled for decades against that inner voice asking for more, this experience can feel almost liberating. And that, in turn, is radically changing the cultural narrative about body weight, personal discipline, and the very origin of overeating.
The Hidden Price: Muscle Mass Loss
This is where the conversation gets complicated. When the body loses weight rapidly —whether due to restrictive diet, bariatric surgery, or medication— it doesn't just lose fat. It also loses lean tissue, meaning muscle. And data from GLP-1 clinical trials raised alarms in the scientific community.

The semaglutide STEP 1 and SUSTAIN 8 trials revealed that approximately 39 to 40% of the total weight lost by participants corresponded to lean mass. A meta-analysis published in 2024, which analyzed 22 randomized clinical trials with 2,258 participants, confirmed that, on average, about 25% of total weight loss with GLP-1 agonists corresponds to muscle mass. These are not minor figures. In a person who loses 15 kg with semaglutide, this can represent between 3.75 and 6 kg of lost muscle.
Muscle is not just a matter of physical appearance. It is the body's most important metabolic organ: it regulates blood glucose, protects joints, supports immune function, and is one of the main predictors of functional longevity. Accelerated muscle mass loss, especially in people over 50, increases the risk of sarcopenia —the progressive loss of muscle associated with aging— and long-term frailty.
That's what starvation does: you lose equal amounts of muscle and fat. And sarcopenia —the loss of muscle mass— is a hallmark of aging and premature death.
The concerning data: how much weight is lost and what it's made of
How much weight is actually lost with semaglutide, and what is that weight composed of? The following chart summarizes the results of the STEP 1 trial —the most cited pivotal study of semaglutide 2.4 mg for weight loss— and reflects the body composition data that the researchers themselves documented in their results.
The problem is not that GLP-1s don't work. Clearly, they do. The problem is that the weight loss they generate, without adequate nutritional strategies, can seriously compromise body composition. A person can reach their "ideal weight" on the scale while losing a worrying amount of muscle. Researchers already have a name for this phenomenon: thin fat or "metabolically obese normal weight" —thin on the scale, but metabolically fragile inside.
What nutritionists say: muscle as a new priority
Given this scenario, dietitians-nutritionists have reacted quickly and clearly. Their message is unanimous: if you are taking a GLP-1, protein and strength training are not optional, they are part of the treatment. The most recent clinical guidelines recommend consuming between 1.2 and 1.6 g of protein per kilogram of body weight per day during treatment, amounts that, paradoxically, are difficult to achieve when appetite is suppressed. This is where the most practical challenge lies: the drug silences hunger, and with it, often also the desire to eat enough protein to protect muscle.

Nutrition professionals also point out another angle that is often overlooked: the quality of what is eaten during the times when one does eat. With reduced appetite, each intake must carry the maximum possible nutritional value. There is no room for empty calories. The body, receiving less total energy, needs that energy to be accompanied by complete protein, essential micronutrients, and enough fiber to maintain gut health. In this sense, active nutritional supervision during GLP-1 treatment is not a luxury or a supplement: it is an indispensable part of the therapeutic protocol.
Conclusion: A Powerful Drug That Needs Company
GLP-1s are, without a doubt, the most transformative pharmacological tool in obesity treatment in decades. They redefine hunger in a way no diet has ever achieved, and their results in weight reduction, glycemic control, and cardiovascular risk are real and clinically relevant. But science is also clear on something fundamental: losing weight is not synonymous with gaining health if that loss is accompanied by a significant amount of muscle mass.
Nutritionists are not against Ozempic. They are against using it alone. The combination of adequate protein, progressive strength training, and professional monitoring is not an extra for those using GLP-1s: it is the difference between losing weight in a way that improves your long-term health, or losing weight in a way that makes you frail. The drug can silence hunger. But preserving muscle, caring for body composition, and building habits that last when treatment is stopped—that still requires strategy, context, and, above all, a nutrition professional by your side.